
“The spirit is willing, but the body is weak”. Matthew 26.41.
 The eyes begin to flicker, the face contorts into a hideous countenance, the toes feel stiff then numb. There is a metallic taste in the mouth, sounds are amplified into the ears, and the arm begins to jerk. A rushing sensation irritates the blood, the lungs suddenly gasp for air, the head vigorously shakes and the lips shout ‘Oh God!’.
The eyes begin to flicker, the face contorts into a hideous countenance, the toes feel stiff then numb. There is a metallic taste in the mouth, sounds are amplified into the ears, and the arm begins to jerk. A rushing sensation irritates the blood, the lungs suddenly gasp for air, the head vigorously shakes and the lips shout ‘Oh God!’.
I ask, “what is wrong with me?”
The neurologist books me in for an EEG scan to test for epilepsy.
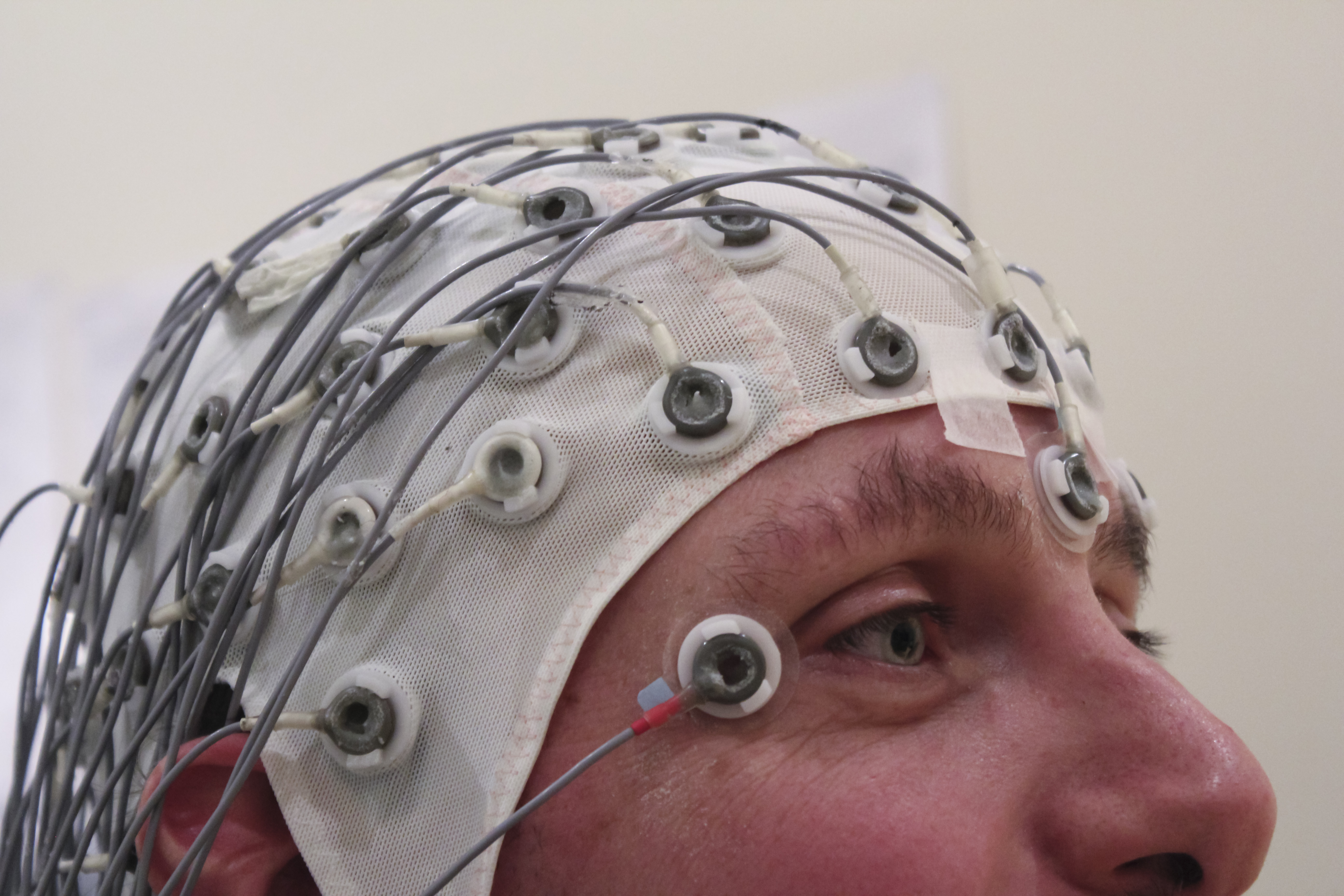
1924 was one of the most significant years in the history of modern neurology. German psychiatrist, Hans Berger, created the Electroencephalogram (EEG), which could detect neurological activity; without intrusive brain surgery. In 1935, Gibbs and colleagues plugged a patient into this machine. The patient had an absence seizure and the first evidence that abnormal neurological activity was the possible cause of seizures was recorded. Repeated studies confirmed such results. Enthused by these findings, clinical EEG laboratories for epilepsy were founded in continental Europe, Great Britain and the United States.
It is 2008. I am hooked up to this machine. Lights flicker. I fall away.
I wake up, I feel drugged, I softly snore whilst making tea. I forget that I am making tea. I sit down. I remember that I am making tea. I stir the tea. The tea is being swished about in a funny jagged motion. I sit down. I raise the cup to my lips. The cup is moved to my cheek. I raise the cup to my lips. The cup is placed on the floor. I go back to bed.
 Such bizarre symptoms were described as long ago as 2000 BC. Accounts written in Akkadian, in ancient Mesopotamia, talk of antasubba or miqtu, noting the sporadic, ”jerky movements” and ”muscle rigidity” observed in people who were thought to have epilepsy. In the Ancient Hindu Medical text of the Sushruta samhita (600BC), written in Sanskrit, symptoms of “numbness (paralysis), convulsive contortions of the limbs (Akshepa), anaesthesia, and various kinds of pain (Sula)” are described. In Ancient Greece, symptoms such as ‘teeth gnashing’, ‘convulsions’, and ‘screaming like a horse, was, when appropriate, given the Greek verb epilambanein (the term from which epilepsy is derived), meaning “to seize, possess, or afflict.”
Such bizarre symptoms were described as long ago as 2000 BC. Accounts written in Akkadian, in ancient Mesopotamia, talk of antasubba or miqtu, noting the sporadic, ”jerky movements” and ”muscle rigidity” observed in people who were thought to have epilepsy. In the Ancient Hindu Medical text of the Sushruta samhita (600BC), written in Sanskrit, symptoms of “numbness (paralysis), convulsive contortions of the limbs (Akshepa), anaesthesia, and various kinds of pain (Sula)” are described. In Ancient Greece, symptoms such as ‘teeth gnashing’, ‘convulsions’, and ‘screaming like a horse, was, when appropriate, given the Greek verb epilambanein (the term from which epilepsy is derived), meaning “to seize, possess, or afflict.”
Today, epilepsy is defined as,
A disease of the brain defined by any of the following conditions,
1. At least two unprovoked (or reflex) seizures occurring 24 hours apart,
2. One unprovoked (or reflex) seizure and
3. a probability of further seizures similar to the general recurrence risk (at least 60%) after two unprovoked seizures, occurring over the next 10 years.
What is interesting about this ‘disease’ is the aspect which has not been explicitly expressed, the unusual involuntary aspect that defines these abnormal behaviours; abnormal because they are not contextually explicable in any everyday sense. For instance, one’s teeth may gnash due to cold weather. But if this were the case it would not be a seizure. Nor does one feel like they are voluntarily gnashing their teeth, as if this were the case, such behaviours would be explicable without invoking pathology. Basically, teeth gnashing is not a sign of disease if it’s cold, or if you are choosing to gnash your teeth.
I ask, “What are the EEG Results?”
The neurologist looks at me with suspicion and replies, “Your results are normal Ms. Elliott.”
Normal EEG results do not necessarily entail the person does not have epilepsy, as people with epilepsy do not always show abnormal EEG recordings, yet they may typify the same clinical symptoms.
PNES relies heavily on EEG scans for its diagnosis
As S. J. M. Smith notes: “It is crucial to recognise that a normal EEG does not exclude epilepsy, as around 10% of patients with epilepsy never show epileptiform discharges.”
However, there are other causes of seizures; for example, spinal-cord abnormalities.
I ask again, “what is wrong with me?”
The neurologist replies, ”You are mentally ill”.
A black hole opens up, and I fall down it.
Does the body rule the mind, or does the mind rule the body?
I am paralysed now, hearing the world go by without me, hearing the world trap me in my body; frozen stiff, for a moment, and then another. My eyes glaze over. The left eye slightly contracts and blurs the world into a grey sky. Someone is shouting at me. Someone is being aggressive towards me. I can’t defend myself. I try. I fail. I stop. I try. I fail. I try. My arms shake under the vacillation of power split and opposed in a fractured world, until they are either brought under the rule of the will, or brought under paralysis by the body. Gradually, I feel like I can exert increasing control over my arms. They feel heavy. I pull myself up using the handle on the oven. Now, my legs.
The idea that mental Illness can cause seizures stems from Sigmund Freud. These bizarre symptoms, according to Freud, were caused by emotions and the unconscious mind (repressed energies and drives), and not organic brain abnormalities. They were called hysterical seizures. They were a way of managing pain, by repressing horrible (often sexual) experiences, and somehow converting those experiences into neurological symptoms. But despite the physicality of the symptoms, they were , nonetheless, caused by psychological phenomena.
I ask, “What is my diagnosis?”
The neurologist replies, “Psychogenic non-epileptic seizures. Formerly known as, pseudo-seizures.”
No further tests are done.
I’m given a leaflet. I am told that I will receive notification of an appointment to see a psychiatrist. I leave the neurologists office. I lock myself in the toilet. I cry alone. Tears fall onto the leaflet. I don’t see the neurologist again. It is 2009. I start a degree in Philosophy at the University of Greenwich.
Selim R. Benbadis, M.D., Director of Comprehensive Epilepsy Program and professor at University of South Florida and Tampa General Hospital, is a leading pioneer in the study of PNES. Benbadis claims that physicians have the ability to diagnose PNES with near certainty by using EEG-video monitoring. He describes PNES as attacks that look like epileptic seizures, but are not caused by abnormal neurological activity. They are manifestations of psychological distress and not manifestations of any abnormalities of the body.
Here, what we have, is a dualistic approach to health. The mind and body are separated. The brain is normal and the mind is abnormal. The mind is abnormal so the body is abnormal.
Needless to say, this diagnoses seemed somewhat premature. Despite the remarkable powers of the EEG machine, an EEG recording does not give a comprehensive detailed illustration of what is happening in the brain. What the diagnoses was based on was the absence of abnormal neurological results, and a picture of the kind of seizures I was having, and their frequency, which differed to the type and frequency of epileptic seizures. But this is a heuristic medical judgement that lacks accuracy. And this judgement also led the neurologist into the realm of the unknown, into the realm of an unconscious, ethereal, neurologically independent mind.
It is 2010. I see a psychiatrist.
Dr. Mellers ask, “Has anything bad or traumatic happened in my life?”
I reply, “Yes”.
Dr. Mellers asks, “Could you tell me what happened?”
Dr. Mellers found that higher rates of abuse were reported in patients with dissociative seizures, in comparison with epileptic controls and unselected psychiatric patients in a number of large studies.
Such events which precipitate dissociative experiences do not exclude traumatic abusive experience in adulthood. So the inference goes, people have neurological symptoms, because they were abused. I was told, this is why I am ill.
 I am in an ordinary chair. A CBT officer is talking to me. The world appears uncanny in its new two-dimensional reality. It is hollow inside this body. Only the broken skeletons of logic manifest in conversation. The eyes are glazed over. I am gone. I realise I am gone. I come back. I am gone again. A rushing sensation irritates the blood, the lungs suddenly gasp for air, the head jolts to the side, the lips mutter, “I won’t come.” I come back. I apologise. The eyes glaze over. I am gone again. Halfway between ‘reality’ and a ‘dream’, the smoke thickens.
I am in an ordinary chair. A CBT officer is talking to me. The world appears uncanny in its new two-dimensional reality. It is hollow inside this body. Only the broken skeletons of logic manifest in conversation. The eyes are glazed over. I am gone. I realise I am gone. I come back. I am gone again. A rushing sensation irritates the blood, the lungs suddenly gasp for air, the head jolts to the side, the lips mutter, “I won’t come.” I come back. I apologise. The eyes glaze over. I am gone again. Halfway between ‘reality’ and a ‘dream’, the smoke thickens.
I sit in that ordinary chair, for over a period of 2 years.
Researching the history and philosophy of PNES
At that time, I was subject to the many conceptual issues that I could not articulate, or were articulated onto ears deafened by their doctrine and prejudice. The beliefs of the medical establishment created an atmosphere around me that painted a picture of madness without form; of an unhinged, detached mind that was unknown to the subject, but known to the other. However, over time, my academic training was refined.

Ellese Elliott
In 2012, I begin an MSc in the Philosophy of Mental Disorder at King’s College London. I study at the place where the idea of PNES is practiced; where I am treated. Many fascinating ideas are learned and produced. However, it is 2014. I still have symptoms.
I ask ‘Why do my symptoms persist?’
Dr. Mellers replies ‘You need to completely accept that this disorder is purely psychological. There is nothing wrong with your brain.’
A lengthy discussion occurs.
I say “I need help.”
Dr Mellers replies, “You are a smart girl. I am sure you will work it out.”
Was my philosophical scepticism really holding me back? Does the cure really lie in dogmatism? I wasn’t about to find out. If my philosophy is preventing me from being cured, so be it. I am not willing to be evangelised by the church of psychiatry just yet.
It is July, and I am told that I can no longer do my dissertation on those occupy London protesters who had been sectioned. I hastily commence an in depth philosophical analysis of seizures, and PNES, under the instruction of Professor Derek Bolton.
There are two main arguments that were employed against PNES within my dissertation, that will now be briefly put forward.
Argument 1.
Imagine the EEG was never invented and that there is no evidence that neurological abnormalities underpin epilepsy. Yet, a fantastic machine has been built, the Elliottanatomater, which detects epigenetic coding malformations in patients with seizures, effecting their nervous-system to contract in certain events and prevents electrical signals from being sent to the right places.
However, there is a problem, not with the machine, but with the person in it. He doesn’t show as being epigenetically malformed. There must be something going on psychologically, away from the world of epigenetics and the organic world generally. He has epilepsy. The psychologists are called and they ask him a number of questions. The psychologists find that these seizures come on when he is stressed (which is known to be a cause of epileptic seizures). Also they find that one third of people with epilepsy are seizure free for at least two years with hypnosis and aromatherapy (smelly oils being rubbed into the skin). We also give him a bit of LCT (life coaching therapy), which has a similar success rate. This must prove that epilepsy is psychological and not physiological, right?
Wrong. This inference is based on the state of technological advancement (the EEG might not be a reliable guide), and doesn’t necessarily mean that the seizures are psychological, not physiological. It also draws upon the seeming positive correlation between certain events and certain symptoms, leaving something important out – the body. This leads us on to the second issue.
Argument 2.
The concept of PNES relies on the untenable notion of substance dualism, where the mind is independent of brain function, and they are considered two separate substances. But who today, in the face of much scientific evidence that consciousness is brain-based, and where there is no evidence or logical proof that the mind is independent, subscribes to this view?
Well, apparently, platoons of psychopathology specialists base their profession on it, and the state spends millions of pounds to such platoons to deal with these abused minds which swim around, unknown to their subject, creating all kinds of havoc.
In a paper entitled, ‘The false organic–psychogenic distinction and related problems in the classification of erectile dysfunction’, Benjamin D. Sachs makes a number of points that can be used against the diagnosis of conversion disorder (according to which physical or neurological symptoms are caused by mental or emotional distress):
Sach’s states that this severance
is based on an obsolete view of mind–body distinctions, does not take into account knowledge of the neurobiology of ‘psychological’ disorders, disregards the fundamental meaning of ‘psychosomatic’, is too often diagnosed by exclusion, and may imply to the patient that his ED (or for our purposes PNES) is ‘all in the mind.’
So there are two schools of thought. The first, held by pathologists, asserts that the mind is only the brain at work, and all mental processes can be explained in terms of brain processes. The other school of thought, held by psychopathologists, holds that there are emergent processes of mind that cannot be altogether explained by brain function.
However, as Sachs’ points out, they both hold that the mind is not something entirely other than brain function. Both seemingly reject dualism.
Experimental psychologists, linguists, anthropologists, and other behavioural scientists all methodologically analyze mental processes, but fail to consider brain function, although they would all be likely to agree that all psychological processes are regulated (at least in part) by brain functions. Therefore, they cannot hold that there can be psychogenic dysfunction without the brain.
There is no PNES. It is simply untenable. And I refuse to give over my reason to such nonsense, in the hope of a cure. Seizures can only occur through the mediation of organic processes.
I am in my house. My friend Eliza is here. We are laughing. I start to feel happiness linger into my heart. She is funny. She is smiling. I laugh harder. A pain creeps into the back of my head. The feeling of happiness intensifies. The pain intensifies. I stop laughing.
There will be better days to come. However, I do not base these days on myths. I base them on philosophy and science. And those days will come soon, when the advancement of technology reveals evidence of micro-neurological abnormalities in patients with so called psychological non epileptic disorder, and psychologists incorporate these findings into their discipline for a more holistic view of what it is to suffer from seizures.
*****
Ellese Elliott has a first-class philosophy degree from Greenwich and an MSc in the philosophy of mental disorder from KCL. She is organizing an event to explore how society makes us sick, on Thursday December 4, in London. Details here.
For a more detailed philosophical investigation on the subject of seizures, click here.
Reference List
Glasser, Gilbert.”Reflections of a Previous Editor of Epilepsia.” Epilepsia 50 (2009):349-350. Accessed August 19, 2014. doi: 10.1111/j.1528-1167.2009.02028.x.
Vannemreddy, P., Stone, J., Vannemreddy, S., Slavin, K. “Psychomotor seizures, Penfield, Gibbs, Bailey and the development of anterior temporal lobectomy: a historical vignette.” NCBI. (2010) : 103-107. Accessed November 09, 2014. doi: 10.4103/0972-2327.64630.
Wilson. J. V., and Reynolds, E. H.. “Texts and documents. Translation and analysis of a cuneiform text forming part of a Babylonian treatise on epilepsy,” Medical history 34 (1990): 185. Accessed August 2, 2014.
Bhishagratna, K. “AN ENGLISH TRANSLATION OF THE SUSHRUTA SAMHITA WITH A FULL AND COMPREHENSIVE INTRODUCTION, ADDITIONAL TEXTS, DIFFERENT READINGS, NOTES, COMPARATIVE VIEWS,
INDEX, GLOSSARY AND PLATES,” Internet Archive(2008). Accessed Novemeber 07, 2014.https://archive.org/stream/englishtranslati00susruoft/englishtranslati00susruoft_djvu.txt
Magiorkinis, Emmanouil., Sidiropoulou, Kalliopi., Diamantis, Aristidis. “Hallmarks in the history of epilepsy: Epilepsy in antiquity,” Epilepsy and Behaviour 17 (2010) 103. Accessed August 9, 2014. DOI: 10.1016/j.yebeh.2009.10.023.
Fisher, Robert S., Acevedo, Carlos., Arzimanoglou, Alexis., Bogacz, Alicia., Cross, Helen., Elger, Christian E., Engel, Jerome Jr., Forsgren, Lars., French, Jacqueline A., Glynn, Mike.,Hersdorffer, Dale C., Lee, B I., Mathern, Gary W., Moshe, Solomon L., Perucca, Emilio., Scheffer, Ingrid., Tomson, Torbjon., Watanabe, Masako., and Weibe, Samuel. “A Practical Clinical Definition of Epilepsy” Epilepsia 55 (2014) 477. Accessed August 12, 2014. doi: 10.1111/epi.12550.
Meythaler, J M., Tuel S M. , and Cross L L., “Spinal Cord Seizures: A Possible Cause of Isolated Myoclonic Activity in Traumatic Spinal Cord Injury,” Spinal Cord 29 (1991): 557. Accessed August 12, 2014. doi:10.1038/sc.1991.81.
Kaplan, Peter and Fischer, Robert. Imitators of Epilepsy. New York: Demos Medical Publishing Inc., 2005. Accessed August 20, 2014. http://books.google.co.uk/books?id=zg5T1CsIj7UC&pg=PT338&lpg=PT338&dq=ancient+greece+epilepsy+and+hysteria&source=bl&ots=6DVPrG9uJQ&sig=m3pVEjO73d2kbN624QTcfNs4KLY&hl=en&sa=X&ei=oIIHVLf1JOSN7AbItIGYCQ&redir_esc=y#v=onepage&q=ancient%20greece%20epilepsy%20and%20hysteria&f=true.
Betts, Tim. “Use of aromatherapy (with or without hypnosis) in the treatment of intractable epilepsy—a two-year follow-up study.” Seizure 12 (2003):534-538. Accessed September 8, 2014. DOI: http://dx.doi.org/10.1016/S1059-1311(03)00161-4
The Truth about Psychogenic Non-epileptic Seizures.” Accessed August 12, 2014. http://www.epilepsy.com/article/2014/3/truth-about-psychogenic-nonepileptic-seizures
“Nonepileptic Seizures.” Accessed August 16, 2014.
Selim R Benbadis Leanne Heriaud . “Psychogenic (Non-Epileptic)Seizures, A Guide for Families & Patients.” http://hsc.usf.edu/COM/epilepsy/PNESbrochure.pdf.
Mellars, John D.C..”The approach to patients with “non-epileptic seizures,” Postgrad Med J. 81 (2005): 498–504. Accessed August 17, 2014. doi:10.1136/pgmj.2004.029785. (My Neuro-psychiatrist).
Sachs, Benjamin D. “The false organic–psychogenic distinction and related problems in
the classification of erectile dysfunction” International Journal of Impotence Research 15 (2003): 72-74. Accessed September 12, 2014. doi:10.1038/sj.ijir.3900952.