
 Åsa Jansson is a Junior Research Fellow at Durham University’s Centre for Medical Humanities. Her current research explores the history of hallucinations and delusions in modern medicine, and is carried out in conjunction with Durham’s interdisciplinary project Hearing the Voice.
Åsa Jansson is a Junior Research Fellow at Durham University’s Centre for Medical Humanities. Her current research explores the history of hallucinations and delusions in modern medicine, and is carried out in conjunction with Durham’s interdisciplinary project Hearing the Voice.
As Nikolas Rose[1] and others have shown, our unprecedented ability to map, codify, record, and modify human biology – what Rose calls ‘life itself’ – is both directed by, and contested within, the political sphere. And if we dig a little deeper we can also start to see how we as subjects, consumers, patients, and citizens internalise the ethos of the prevailing economic system – free market capitalism – and the neoliberal ideology that underpins it.
In other words, neoliberalism operates not only at the level of government, business, or finance, but permeates our everyday lives and shapes our selfhood. Its value system informs our perception of health and illness: what it means to be healthy, who and what is constituted as pathological, and how we should prevent and address pathology. This is particularly evident in regard to current models of mental illness.
At present, mood disorders such as depression and anxiety disorders are primarily seen as internal and individual problems to be solved at the individual level. Morbid emotionality is a maladaptive response by the individual to their environment, meaning that the management of distress becomes an individual responsibility, rather than a social one. Thus, an individualised, neurobiological model of psychological distress sits comfortably within a political framework that emphasises individual responsibility and choice over social support.
In this context, the favoured treatment for affective disorders is antidepressants (SSRIs) or Cognitive Behavioural Therapy (CBT), or a combination of the two – treatments which are comparatively cost-effective and which focus on the individual brain and mind as the site of pathology.
A key strategy of CBT and its sister-treatment Dialectical Behaviour Therapy (DBT) is ‘emotion regulation’. The idea is that through persistent practice, we can learn to intervene in and successfully regulate disproportionate, distressing, and irrational emotions.[2] The concept of emotion regulation is premised on a model of emotion as automated and involuntary, but nevertheless an event, or process, that can be regulated.
There is a subtle tension that arises from this model, one between the biologised mind as morally neutral, and social conduct as an extension of the biological mind, conduct that possesses an unequivocal moral quality – in short, between the internal (biological) production of emotion and its external (social) manifestation. In order to understand this tension and the work it does in relation to the neoliberal ethos, we must trace our current modern models of affect and conduct to their roots in nineteenth-century science and medicine.
For the Victorians, the biological mind co-existed quite comfortably with a Christian doctrine of morality centred upon respectability, responsibility, and self-help, values that were infused with the logic of industrial capitalism and liberal rationality. The idea that emotion is an automated physiological process that can nevertheless be regulated and (more or less) permanently modified over time, arose as Victorian medical scientists attempted to restore a notion of free will, which they were unwilling to dispense with for moral and political reasons, within an epistemological system that held all mental activity to be physiological and potentially reflexive, or automated.
In the early nineteenth century, increasingly advanced technology equipped medical scientist with new ways of seeing the brain. Psychiatric autopsies appeared to hold the promise of postmortem diagnoses applied with far more accuracy than medical judgment based only on observation of and communication with living patients.[3] But some types of mental disease consistently failed to turn up lesions visible even under a new generation of microscopes – these were primarily different types of ‘affective (or emotional) insanity’ where the intellect was largely unaffected.
This did not sit well with an emerging medical speciality that was intent on demonstrating its scientific credentials. Thus, in order to explain the unseen operations of the mind, including these elusive forms of insanity, in scientific language, Victorian alienists (psychiatrists) borrowed concepts from experimental physiology.
At the time, physiologists were carrying out pathbreaking (and, for the living animals on whom they experimented, brutal) research into reflex action – the physiological process whereby stimuli applied to nerves triggers automated muscle activity. Most scientists argued that this type of reaction didn’t involve the ‘higher’ realm of the brain, which was responsible for conscious thoughts and exercising of the will.
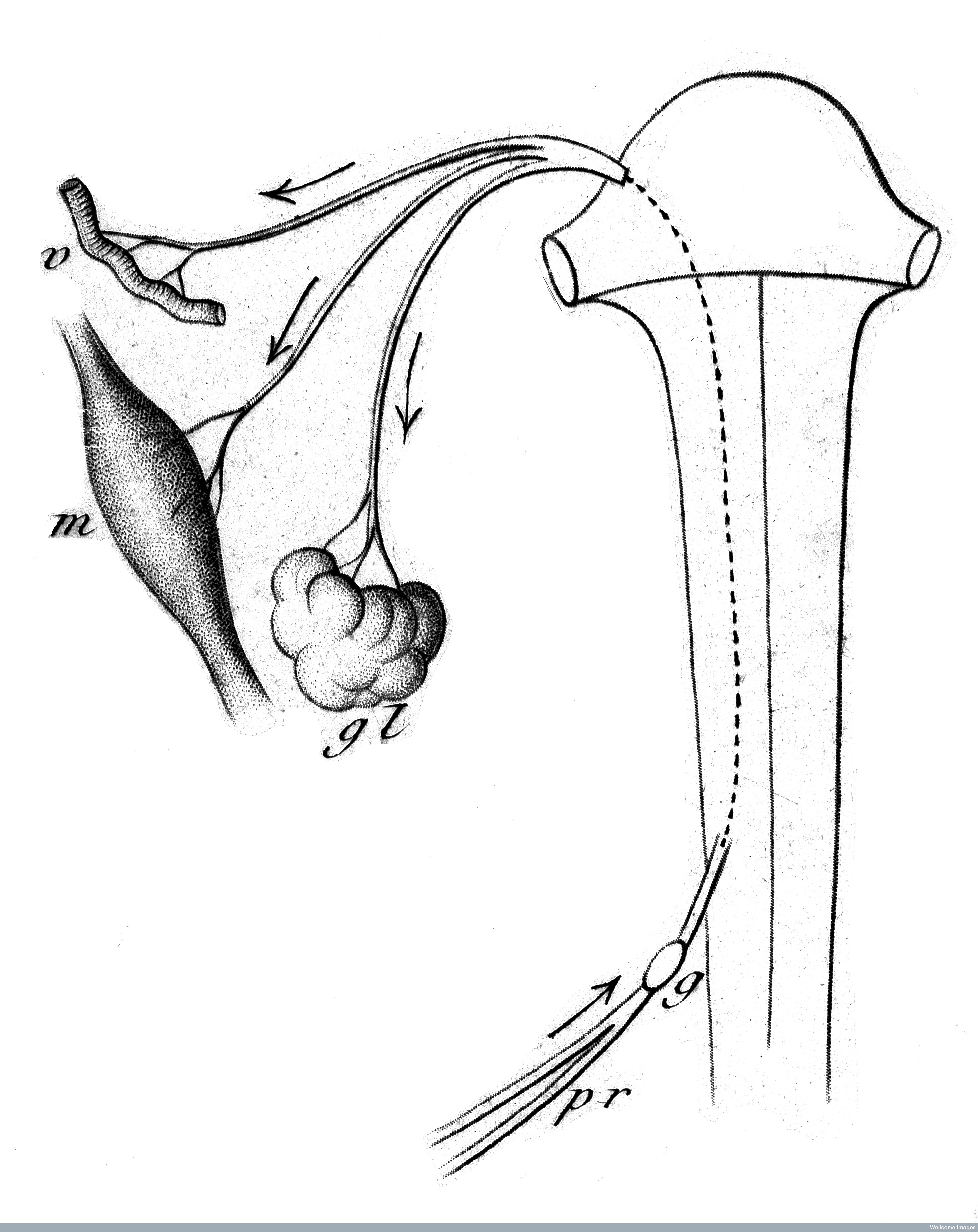
Diagrammatic representation of reflex action, from Charles-Edouard Brown-Sequard’s Course of Lectures on the Physiology and Pathology of the Central Nervous System (1860). Credit: Wellcome Library, London
However, in the 1840s, British physician Thomas Laycock and German psychiatrist Wilhelm Griesinger both argued that the kind of reflexive action applied to sensory-motor activity also applied to the realm of thoughts, emotions, and volition (the will).[4] They both suggested that there was a form of psychological reflex action which was analogous to the physical (muscle) reflex, and which could be triggered not just by external stimuli, but also by thoughts and abstract sensations. This argument had vast repercussions for the sciences of mind and brain, and formed the basis for the modern concept ‘disordered emotion’.
Many British alienists drew on these ideas in order to explain how mental disease emerged and progressed. However, the new physiological model of mental activity called into question the power of agency, particularly for medical scientists who perceived all mental activity as reflexive physiological reactions.
For instance, prominent alienist Henry Maudsley argued that involuntary psychological reflex action could take place both with or without conscious awareness, and that insanity could compromise a person’s ability to exercise their will, even in cases of emotional insanity where sufferers were still capable of rational thought.
While he rejected the possibility of free will on physiological grounds, Maudsley was unwilling to let go of it entirely, as this would suggest that ‘Man’ was incapable of self-control, for Maudsley a morally untenable position. In order to revive a notion of independent will linked to moral conduct, he turned to the idea of habit. Drawing on the work of psychologist Herbert Spencer and others, he argued that not only actions, but also ideas, emotions, and general character could be habitually developed. For instance
A passionate person who has by patient watchfulness over himself and by a course of steady perseverance and practice accustomed himself to wear an outward air of calmness and to speak in quiet, measured language when he is inwardly in a towering passion, making thus a clever art of his natural defect – as it is the part of wisdom to do with all natural defects – succeeds in making that regulated discharge of energy the habit of his life, and in the end does it quite easily.[5]
Importantly, the development of mental habits was, for Maudsley, a physiological process, whereby habit became a psychological reflex – in other words, when emotional regulation, or control, was practiced to perfection, it would become automated, reflexive.
Henry Maudsley. Credit: Wellcome Library, London
In this way, a physiological conception of mental activity didn’t erase moral responsibility and conduct, it reinforced them. This was also true in terms of mental disease. While Maudsley believed that people who became insane generally had a hereditary predisposition, he argued that each individual could act to prevent themselves from deteriorating in this way. Similarly, the ability to exercise the will played a key role in recovery from mental disease, which was in the first instance marked by ‘a revival of the power of will’. This was particularly true in the case of affective insanity, where only the emotions were disordered.[6]
These ideas became increasingly popular toward the end of the century, as scientific writers tried to navigate and mediate between the deterministic view of human nature espoused by degeneration narratives, and a belief in human betterment and individual responsibility.
Maudsley’s work reflected contemporary cultural views on character, respectability, and moral agency, illustrated by the popular doctrine of ‘self-help’ most famously espoused in Samuel Smiles’ book of the same name. Self-Help was a Victorian bestseller and a libertarian manifesto that rallied against ‘over-guidance and over-government’ and argued that the way to generate positive social reform was ‘by better habits, rather than by greater rights’.[7]
The way to improve one’s character was, Smiles argued, through the development of ‘good habits’, which required constant ‘watchfulness’ and ‘regulation’ of thoughts and actions, but once fully formed, ‘habit acts involuntarily and without effort.’ According to Smiles, there was no virtue or state of mind that could not be deliberately formed through significant and persistent effort. Thus, in a turn of phrase that resonates with twenty-first century lifestyle philosophies, he concluded that ‘even happiness itself may become habitual.’[8]
Smiles also argued that ‘self-regulation’ played an important role in strengthening the nation state and the economy, as it promoted industriousness. The language around self-regulation exemplifies how the new sciences interacted with contemporary language around industrial capitalism. Roger Cooter has explored the close relationship between physiology and capitalist economics in the early nineteenth century, arguing that despite its inability to offer prescriptive health advice, physiology appealed to a popular audience, and that its value lay in providing a set of ‘laws of life’ which explained liberal-capitalist society and its consequences as natural and self-regulating.[9]
That is, it presented an image of society in which individual prosperity and a better life came about through habitual self-regulation, in the same way as an economy that was allowed to self-regulate would prosper and grow. In other words, it promoted an agenda fundamentally opposed to radical social intervention, in people’s lives as well as the economy.
Self-regulation – of both the market and of the mind – has made a forceful comeback in contemporary Western society. But, much like in the nineteenth century, a process conceptualised as ‘natural’ nevertheless warrants intervention at times of malfunction, in order to restore its natural flow and functions. Within a twenty-first century model of the biologised mind as an internal, self-regulating system, the behavioural therapies can be conceived of as the intervention that is sometimes necessary in order to restore healthy function. An important consequence of this is that the psychological distress that behavioural therapies are perceived to treat through cognitive and emotional regulation are detached from the social and economic events that, according to a different narrative, could be plausibly posited as the cause of mental distress.
Joanna Moncrieff has noted how the biochemical model that underpins the rationale for antidepressants chimes with ‘the neoliberal values of competitiveness and consumerism’.[10] In a similar way, ‘emotion regulation’ is tied to ideas about individual responsibility and self-help, and offer an equally – if not more – powerful justification for neoliberal ideology, reflecting as it does nineteenth-century ideas of psycho-physiological ‘habit’ and restoring agency – or, if you like, self-help – as the main bulwark against and treatment for psychiatric illness.
My critique is not, however, aimed at the behavioural theories themselves. What I have tried to do in this post is to bring into focus their present relationship to a specific political and moral framework, a relationship that is not inevitable but the consequence of the fusion of certain ideologies and value systems with a particular model of mental activity in the nineteenth century, a situation that results from Victorian scientists’ attempt to reconcile their scientific materialism with society’s prevailing moral codes. It follows that in a different kind of society, we might imagine that these – incredibly useful – therapeutic strategies could be underpinned by a recognition of the socio-economic roots of much psychological distress and work in conjunction with interventions that seek to reduce stress related to work or unemployment and poverty, as well as distress resulting from racism, sexism and so on.
However, by locating psychological distress solely within the individual, and focusing on teaching individuals to regulate their emotions and thus learn to adapt to a triggering environment, without sufficient attention to that environment as a site of pathology, our current framework for explaining and treating mental distress obscures its socio-economic context. This ensures that questions about collective responsibility for psychological well-being that link the latter to socio-economic factors and social justice are foreclosed, marginalising alternative treatment models as well as arguments for radical economic and social reform as the best way to prevent or redress human suffering.
This blog post is based on a paper presented at the Northern Network for Medical Humanities Research Inaugural Congress, held at Durham University on September 14-15, 2017. I explore the relationship between neoliberalism and Dialectical Behaviour Therapy in an article on DBT in Swedish psychiatry, which is a forthcoming in a special issue of the History of the Human Sciences on the history of psychotherapy in Europe.
[1] Rose N (2007) The Politics of Life Itself: Biomedicine, Power and Subjectivity in the Twenty-first century. Princeton, NJ: Princeton University Press.
[2] Gross JJ (1998) ‘The Emerging Field of Emotion Regulation: An Integrative Review’, Review of General Psychology, 3(2) 271-299; Papa A, M Boland , and MT Sewell (2012) ‘Emotion regulation and CBT’, in Fisher JE and O’Donohue WT (eds) Cognitive Behavior Therapy: Core Principles for Practice. Hoboken, NJ: Wiley.
[3] For a comprehensive discussion of psychiatric autopsies in nineteenth-century British asylums, see Andrews J (2012), ‘Death and the Dead-House in the Victorian Asylum: Necroscopy versus Mourning at the Royal Edinburgh Asylum, c. 1832-1901’, History of Psychiatry, 23: 6-26.
[4] Griesinger, W (1843) ‘Ueber psychische Reflexactionen: Mit einem Blick auf das Wesen der psychischen Krankheiten’, reprinted in Gesammelte Abhandlungen, Ersters Band: Psychiatrische Abhandlungen. Amsterdam & Berlin: E.J. Bonset, 1968; Laycock, T (1845) ‘On the Reflex Function of the Brain’, British and Foreign Medical Review, 19: 298-311.
[5] Maudsley H (1884) Body and Will. New York: D. Appleton & Co, p, 93.
[6] Maudsley H (1874) Responsibility in Mental Disease. London: Henry S. King, pp. 270-271.
[7] Smiles S (1876) Self-Help, with Illustrations of Conduct and Perseverance (2nd ed). London: John Murray, p. 2.
[8] Smiles S (1859) Self-Help, with Illustrations of Character and Conduct. London: John Murray, p. 2., pp. 319-322.
[9] Cooter R (1979) ‘The Power of the Body’, in B Barnes and S Shapin, eds., Natural Order: Historical Studies of Scientific Culture. London: Sage Publications.
[10] Moncrieff J (2006) ‘Psychiatric drug promotion and the politics of neoliberalism’, British Journal of Psychiatry, 188: 301-302.